



The 8th Congress of the SEHER (Spanish Wound Healing Society) has just been held in Madrid https://www.congresoheridas.com/index.php/programa. Once again, this scientific meeting has been a meeting point for colleagues and friends. The star novelties of last year’s congress, such as topical sevoflurane in wounds or the App Wound-Registry have been kept among the leading topics in this edition.
It was a pleasure to moderate and participate in a session dedicated to Dermatology in the world of wounds. This year I decided to talk about the interest of early punch grafting in arteriolopathic ulcers, something I love and what I have recently talked about in the blog (“Large leg wounds after mild trauma”)
But what I really loved was to hear and see the excellent results of other colleagues with punch grafting in recalcitrant wounds. This simple, economic and very effective treatment has more and more presence in posters and communications of this congress.
To encourage you to start applying the technique and not to be discouraged when the first dressing changes do not look the way you expected, here I answer the 10 questions that arise most frequently.
-
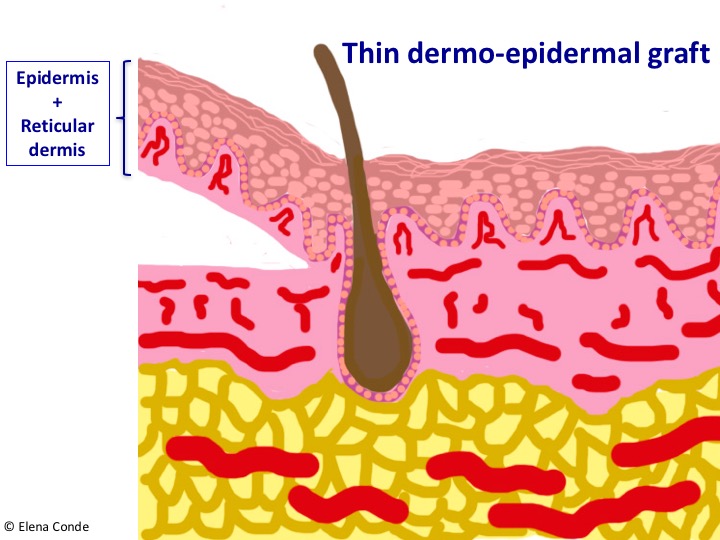
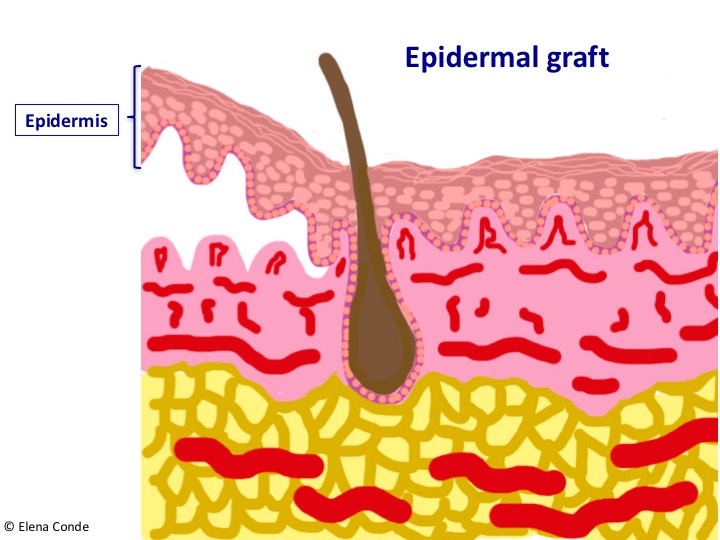
Are these grafts similar to epidermal grafts obtained with the marketed product?
No, they are different. Punch grafts consist of epidermis and superficial dermis, therefore, in the donor site there is a point-like bleeding and when placed on a wound bed in good conditions is produced, graft taking is expected to occur. Epidermal grafts only consist of epidermis, so there is no bleeding after obtaining them, but when they are placed in the wound there is no graft taking and epithelialization is promoted by cells and growth factors released in the bed. I encourage you to read the blog entry in which I explain it in detail: “Differences between epidermal and dermo-epidermal punch grafts”
-
Should I suspend oral anticoagulants before performing the technique?
Since this is a surgery with low bleeding risk, we usually do not suspend them. However, before performing the grafts it is important to ensure that there is good control of the anticoagulation state (INR must be in the expected range).
-
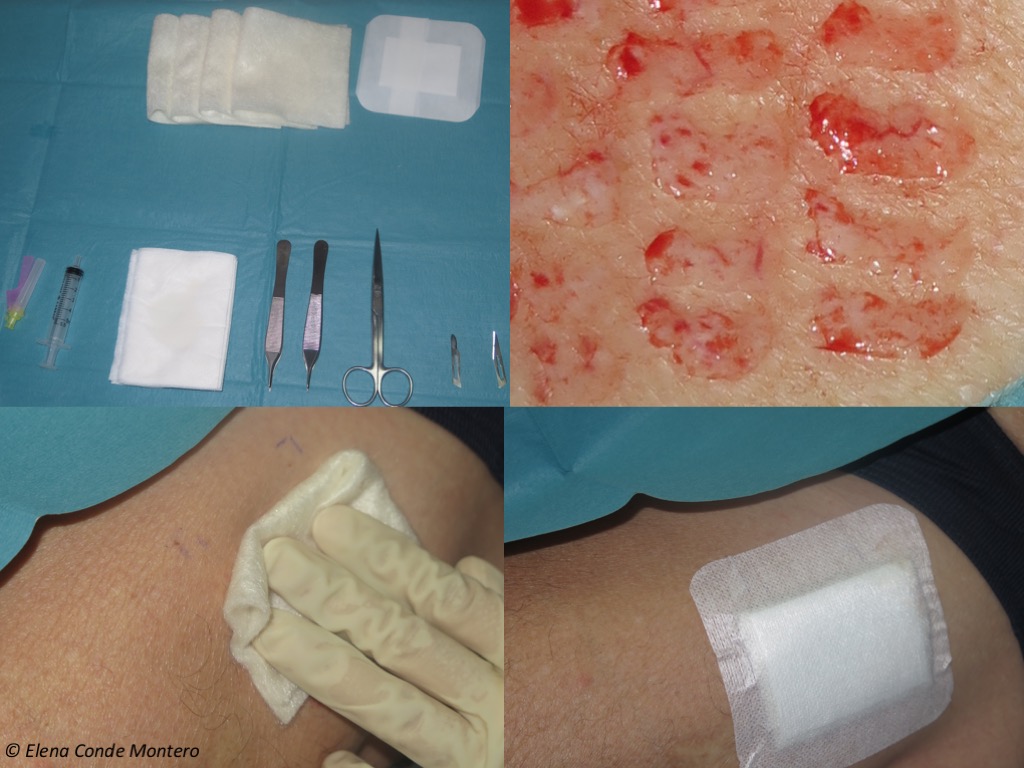
How do I obtain grafts from the donor site?
We usually obtain them from the antero-lateral aspect of the thigh. We infiltrate tumescent anaesthesia with 1% lidocaine diluted with physiological serum.
The grafts may be obtained with punch, curette or scalpel blade. This last system is the one we currently use most frequently.
It is a technique very well tolerated by the patient and we carry it out in the consulting room.
See post “Types of skin grafts to cover chronic wounds: Which one should you choose”
-
What is the expected evolution of the donor site?
Let´s see an example. Immediately after obtaining the grafts, we cover the donor site with calcium alginate and use gauze as a secondary dressing. In this case the first dressing change was carried out on the third day and the donor site as covered again with alginate. One week after the procedure, with scab formation, it was recommended the daily application of a repairing cream with zinc (See post “Why do we use topical zinc on wounds and perilesional skin?”)
In the entry “Which dressing should I choose to cover the skin graft donor site?” you can find more information about the local care of the donor area.

-
What dressing should I use to cover the grafted wound?
We usually cover the grafted area with sheets of calcium alginate, as I have told you in the entry “Why do we use so many alginate sheets in our wound clinic?”. Another option is using interfaces (we mainly use a mesh with lipido-colloid technology and anti-metalloproteinases activity) as primary dressing, and alginate sheets as secondary dressing. In special locations, such as the scalp, flexible foam dressings with adaptable edges are useful to avoid bulky bandages.

-
When is it useful to combine punch grafts with negative pressure therapy?
Negative pressure therapy can help improve the wound bed before graft coverage, but it is also very interesting for promoting graft attachment (especially if wound bed conditions are bad or in special locations, such as the Achilles tendon). You can read more at “Punch grafting and Negative Pressure Therapy: A Successful Couple”


-
What types of wounds can benefit from this technique?
Any wound in which epithelialization is not achieved, provided that there are no signs of infection, the etiological treatment has been optimized and the patient is not a candidate for other reconstructive surgical procedures.
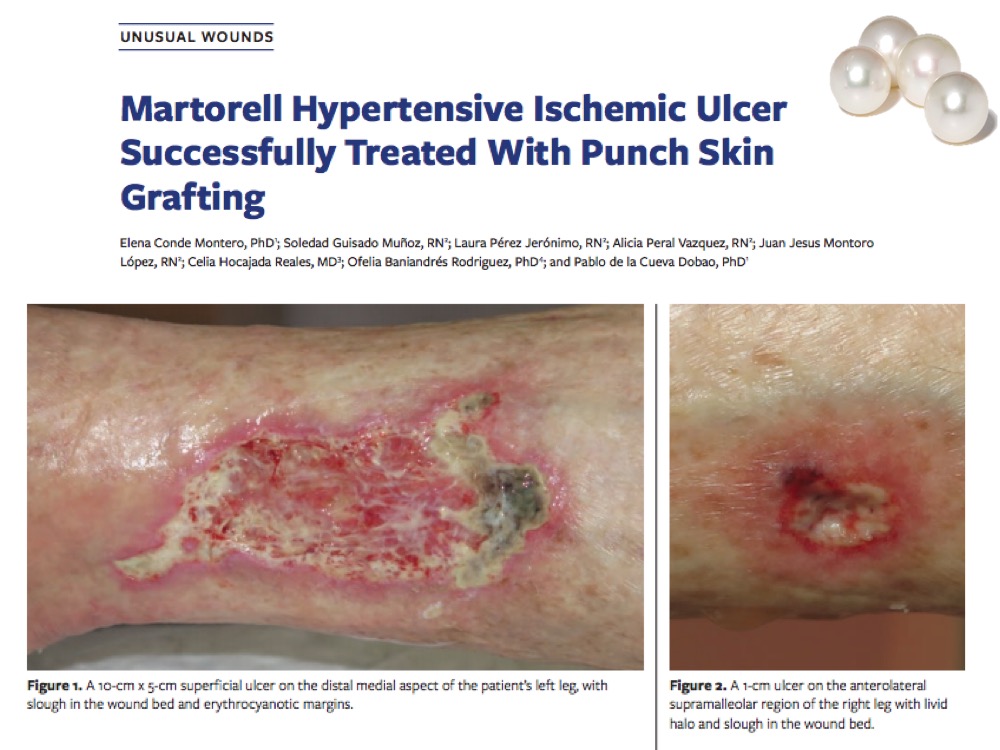
The spectrum of arteriolopathic ulcers, which includes Martorell ulcer and post-traumatic wounds in the context of age-associated arteriolosclerosis, this early treatment is of high interest for, in addition to promoting healing, reducing pain and avoiding lesion progression (See entry: “Large leg wounds after mild trauma”)
-
Is it possible to cover sloughy wound beds with punch grafts?
The ideal situation is to graft optimal beds with red granulation tissue. However, our patients are usually older, with multiple comorbidities, associated pain and anticipatory anxiety for dressing changes. Although we try to improve wound bed tissue as much as possible, it is not always easy to achieve optimal conditions for graft coverage. However, experience tells us that, despite devitalized tissue in the bed and the absence of complete graft taking, the wound benefits from this coverage. Punch grafts behave like independent micro-islands, so those that do not take do not affect the rest and are also beneficial because they can release cells and growth factors interesting for healing. In addition, the analgesic action of these grafts must be underlined, which, as we observed in our clinical practice, is independent of the percentage of graft taking. See post: “Interest of early punch grafting in Martorell hypertensive ischemic ulcer”.


-
How is the expected evolution of the grafted wound?
It varies greatly depending on the characteristics of the wound bed, the wound evolution time, the co-morbidities of the patient and the immobilization of the grafts the first few days after coverage. This immobilization is achieved with local pressure. In leg wounds we put compression bandages and recommend rest with the limb elevated during one week, which is essential during the first 3-4 days.
It is also key to space dressing changes as far as possible and to be as conservative as possible in wound bed cleansing, without removing the grafts that have not taken or the gelled or crusty material that appears between them. IN EACH DRESSING CHANGE WE REMOVE WHAT IS NOT INTERESTING FOR THE WOUND, BUT ALSO GROWTH FACTORS AND CELLS THAT ARE PROMOTING HEALING!
This is the clinical aspect during weekly dressing changes after punch grafting a venous ulcer in the inner aspect of the right leg, of three years of evolution. The whitish colour in the perilesional skin is due to the zinc barrier product we use (See post “Why do we use topical zinc on wounds and perilesional skin?”)
-
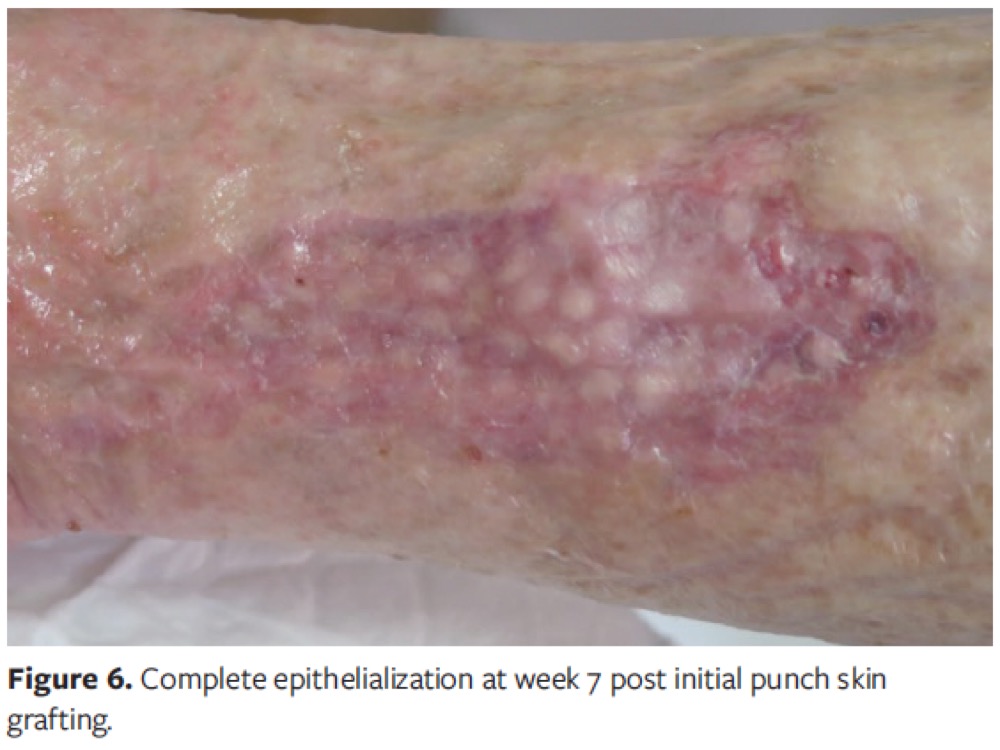
If no graft taking has occurred , is it a total failure?
Quite the opposite. In fact, on many occasions we graft wounds with the sole aim of reducing pain. In addition, when we graft beds with abundant slough, even though no graft taking exists, neoangiogenesis is produced, which improves granulation tissue, and cells and growth factors that promote wound contraction are released. In these cases, we have to perform several sessions of punch grafting to obtain complete epithelialization, something very well accepted by the patient.
I would like to end with heartfelt congratulations to my great colleague and friend, Laura Pérez Jerónimo, for the second prize in Clinical Cases that she received at the 8th SEHER Congress. As could not be otherwise in our practice, this case was treated with punch grafts. You can see her in the photo with Alicia Pérez Vázquez and Lorena Recarte Marín, excellent colleagues and friends too. Congratulations, team!

Also available in: Español (Spanish)


