



The following mental association is very common: “acute wound = wound that will close without problems”. However, an acute wound can become complicated and chronic (or even considered chronic from the moment of its onset due to comorbidities of the patient).
The essential difference between an acute and a chronic wound is that the former will heal in the expected time, while the latter presents a pro-inflammatory microenvironment that prevents the progression of the different phases of wound healing.
While for chronic ulcers there are multiple clinical guidelines, for the management of acute wounds there are no agreed protocols. In fact, the variability in the treatment of these wounds is noteworthy, especially the most frequent ones, which are abrasions, lacerations or superficial ulcers after mild trauma (which are often consulted by Whatsapp and we do not know what to recommend). Therefore, although some of the points in this post have already been covered in other entries, I think that having this “list of tricks” can be very useful to you 😉 Here we go!

- In clean acute wounds, we must avoid aggressive cleansing, with excessive friction. Not only is it not known whether it is better to wash with or without soap, but, as we saw in the post “The art of wound cleansing”, the cleansing of these wounds does not seem to be associated with a lower rate of infection or other healing benefits. In fact, some experts only recommend cleansin dirty wounds (see post “Why do we continue to use topical antibiotics in clean wounds after dermatologic procedures?”)
- If the scab does not fluctuate and there are no signs of infection, we should not remove it. Keeping it hydrated, for example with jelly petrolatum can accelerate the healing process (See post “How do we manage clean wounds after dermatological procedures?”). The use of products with hyaluronic acid (“Reasons for the hyaluronic acid boom in wound healing”) or zinc (“Why do we use topical zinc on wounds and perilesional skin?”) can also help accelerate epithelialisation.
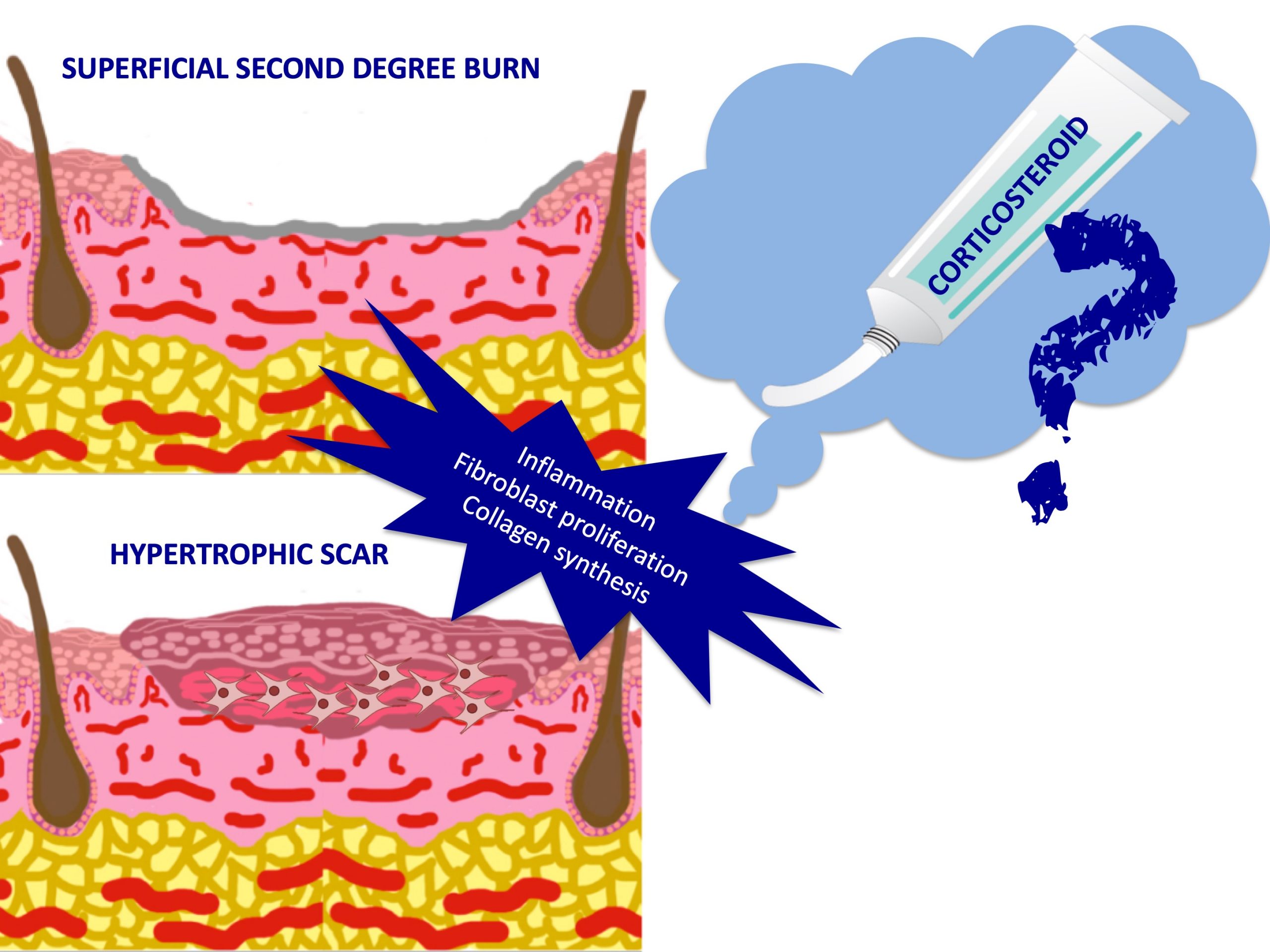
- Superficial burns are characterised by excessive inflammation. This prolonged inflammatory phase not only delays the healing process but also increases the risk of hypertrophic scarring. Although more studies are needed, topical corticosteroids is a very interesting treatment alternative (See post: “Does it make sense to apply topical corticosteroids to improve the healing of superficial burns?”)
4. In clean acute wounds the use of topical antiseptics and antibiotics is of no interest (See post “Why do we continue to use topical antibiotics in clean wounds after dermatologic procedures?”)
5. In superficial exuding wounds, zinc sulphate foments 1:1000, once or twice a day, are of interest because of their astringent power (see post: “Gauzes soaked with astringent and antiseptic foments for wounds and perilesional skin”)
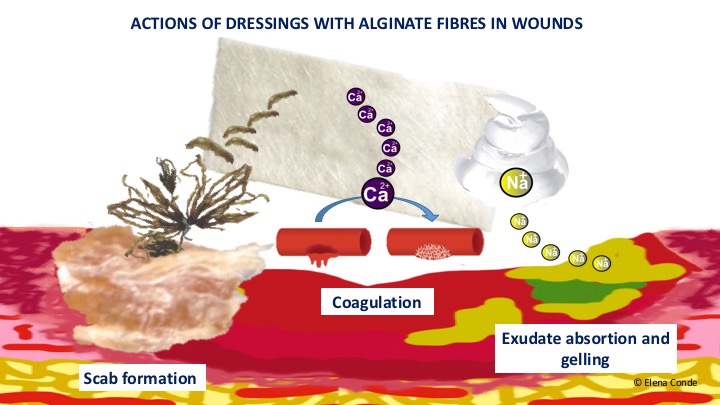
6. No dressing has shown superiority over the others (in fact bioactive dressings are mainly used, in the clinic and in research studies, in chronic ulcers). However, in bleeding wounds, calcium alginate is very beneficial because of its haemostatic power and its ability to “simulate a physiological crust” (See post: “Why do we use so many alginate fibre sheets in our wound clinic?”).
7. If coverage with dressings is required, dressing changes should be spaced as far apart as possible (depending on exudate and discomfort control). We must remember that at each dressing change we remove the excess exudate and denatured tissue, but we also remove growth factors and cells that promote healing).
8. As long as there are no contraindications (see post “New recommendations about compression therapy”), any acute leg wound will benefit from compressive therapy, because of its anti-gravity and anti-inflammatory effect, even if the person does not suffer from chronic venous insufficiency. (See post “Compression therapy after dermatologic surgery on the leg”). We will also recommend anti-oedema measures, such as rest with elevation of the lower limbs.

9. We will avoid the tension forces that separate the edges of the wound, since they make it difficult to contract the wound and promote the appearance of a pathological scar (see post “The myofibroblast: the great ignored in wound healing”).
10. Finally, remember that the evolution of a wound will always depend on the comorbidities of the patient (smoking, age, immobility, nutritional status, cognitive degeneratio, dermatoporosis, chronic venous insufficiency, diabetes…). Therefore, there are wounds that, despite starting out as minor injuries, after trauma that are sometimes so minor that they are not even remembered, should already be considered as ulcers that are going to have a torpid evolution (See posts: “Wounds secondary to dermatoporosis or chronic skin insufficiency”, “Large leg ulcers after mild trauma “).
Also available in: Español (Spanish)


