



I’ve wanted to talk about this “dermatological” practice for a long time. I say “dermatological” because astringent and antiseptic products are a very widespread and effective practice in the treatment of exudative dermatoses. How useful is 1:1000 zinc sulphate solution in the vesicles and erosions of acute dermatitis or 2% sodium borate solution in diaper dermatitis! In the wound healing field there is very little described about the benefit of these solutions, but in our practice how we like zinc sulfate foments in exuding wounds and their macerated and eczematized perilesional skin!
As many of you will not be familiar with these treatments, we will start the explanation from the basics.
How can an astringent and antiseptic solution be applied?
A compress soaked in the solution is applied to the skin. The prolonged contact of this compress with the skin facilitates the penetration and, therefore, the action of the active principle of this solution. The adjective astringent refers to the drying action of this solution and antiseptic to its destructive or inhibiting power of different microorganisms, with low toxicity for our cells.
These aqueous solutions are obtained by dissolving the powdered presentation of the active ingredient in water, something that, depending on the substance, can be done by the patient himself or has to be prepared by the pharmacist.
A small reminder for those of you who are not clear about the indication of the different pharmaceutical forms: in very exudative lesions or in folds, powders in aqueous solutions must be applied to favour their drying, while in very dry lesions, ointments must be used to increase their absorption and hydrate the area. Creams are between these two extremes and their characteristics vary according to the percentage of water and fat they have.
What types of solutions with these characteristics can we use?
If one wants to review the astringent and antiseptic solutions, references in articles and books on wounds and healing are practically non-existent, so one must go to the dermatology or pharmacology manuals.
In fact, I have only found a couple of articles that comment on the interest of potassium permanganate in wounds.1 Of the rest, nothing, but here I present those that we use most frequently in exudative lesions in dermatology.
- Zinc sulphate: this is the one we mainly use in our clinic, where we see predominantly leg wounds. Zinc can be combined with copper and aluminium to enhance its action. The antiseptic action of these three metals is due to their combination with the sulfhydryl group of certain enzymes, thus preventing the proliferation of microorganisms that depend on sulfur oxidation. These metal ions bind to human proteins, modifying their structure and causing them to precipitate. At low concentrations (1:1000), this denaturation and precipitation of proteins means that the ions do not penetrate deep tissues and their astringent action is produced. However, the high concentration of these metals is cytotoxic, as it damages the membranes and intracellular structures, and has a caustic activity.1
- Boric acid: This acid has a predominantly antifungal action. It is not a fungicide, but slows fungal growth. In aqueous dilutions it increases its bacteriostatic power.1 There is a lack of evidence to support its use, but experience tells us that it is very interesting for very wet lesions where there is a risk of Candida We normally use 2% sodium borate, which we obtain by masterful formulation.
- Potassium permanganate: as I mentioned, this is the only one of which there are punctual references in the scientific literature for its use in wounds. I have never used it. Its antiseptic action is due to its oxidizing power.1 By releasing oxygen, it oxidizes the nucleus and intracellular substances of the bacteria, and it also has astringent and deodorant power. To avoid irritation or even burns, it should be used at low concentrations, usually 1:10000.
In published cases, predominantly in cellulitis and acute eczema, which show the benefit of potassium permanganate foments, a steroid cream is also used, so it is difficult to determine the actual benefit of the solution.1
There is controversy regarding its interest in wounds, as many practitioners consider it to be an outdated practice and argue that there are other products that are safer and more effective.2
How are these solutions applied?
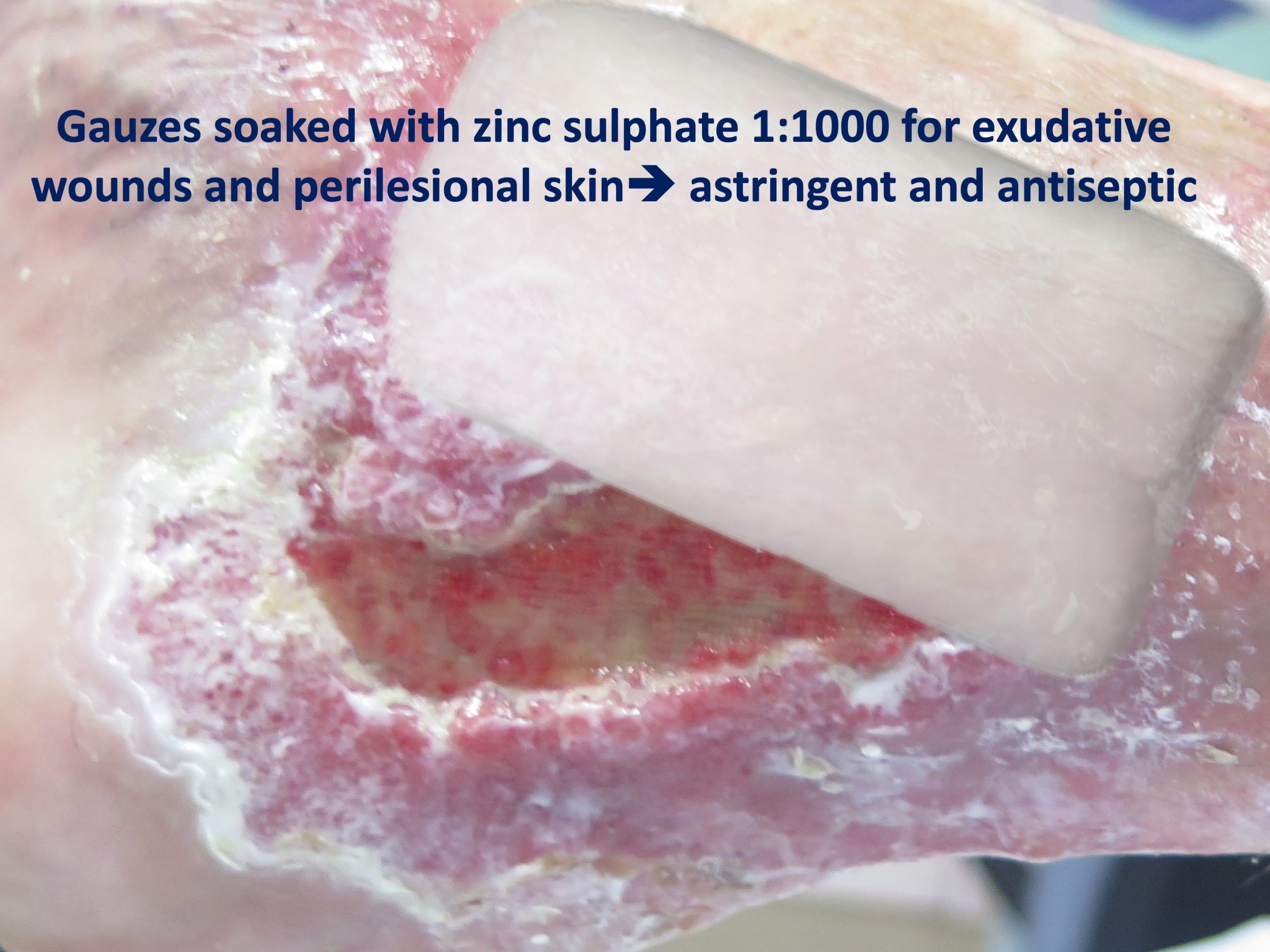
After soaking the gauzein the solution, we keep it on the wound and perilesional skin for approximately 10 minutes. Is this time sufficient? Wouldn’t longer contact be interesting? The problem with keeping the gauze longer is that it can lead to excessive absorption of the fluid by the tissue and worsen the exudate and maceration.
We use 1:1000 zinc sulfate in our clinical practice. To obtain this we dissolve a sachet of 1 g of zinc sulphate in 1 litre of water.
The ideal would be an application every 12 hours, as recommended by dermatologists for acute exudative lesions. However, in leg wounds, except in cases where the patient wears a compression stocking, the frequency of application must be adapted to that of the change of bandage. It is time to remember that if the wound exudate is not controlled, with secondary damage to the perilesional skin, the first thing to do is to think about what is failing: is the compression adequate? does the patient comply with the anti-edema measures we recommend? are there signs of infection? is the dressing adequate?
The combined application, first the astringent solution (in our case usually zinc sulfate) and then the topical corticosteroid cream, is something very used in our wound clinic, with excellent results. This is a widespread practice among dermatologists, especially in acute eczema, but isn’t the eczematized perilesional skin of our venous ulcer patients a dermatological problem that can benefit from this strategy?
As we commented in the post “Why do we use topical zinc on wounds and perilesional skin”, while zinc sulphate is used predominantly as a drying and antiseptic, zinc oxide is of greater interest in promoting healing. Therefore, after gauzes soaked with zinc sulphate, we apply zinc oxide barrier cream to the edges of the wound, which in addition to protecting the skin also promotes its repair. As you can find in this post about zinc, the combined application of topical corticosteroids and zinc oxide increases the beneficial effect of zinc.
Undoubtedly, the use of these solutions in wounds and perilesional skin is a therapeutic strategy with little evidence. Do you have any experience?
References:
- https://en.wikiversity.org/wiki/Antimicrobial_Agents_I
- Anderson I. Should potassium permanganate be used in wound care? Nurs Times. 2003 Aug 5-11;99(31):61.
- Using potassium permanganate for wound cleansing. Readers’ Questions. Journal of Wound Care1994 3:4,
Also available in: Español (Spanish)


