



I have just returned from the joint EWMA& Journées Cicatrisations 2022 congress held in Paris. I thought I would dedicate a post to the new technologies that have been presented and are already available on the market. I would have to talk about cold plasma, phototherapy, electrical stimulation, oxygen therapy, new skin substitutes, sensors for the early detection of pressure ulcers, thigh compression device as an adjuvant to leg compression…. However, I have decided to leave these innovations on hold until such time as I have some experience with some of them and can share my experiences with you:)
As you know, I love the necessary innovation, but I also believe that it is essential to rescue traditional products and practices that have proven to be efficient. It is not because a therapeutic strategy is “old” that it will be worse than a new one. Although I have already dedicated separate blog posts to them (“Why do we use so many alginate fibre sheets in our wound clinic?”, “Why do we use topical zinc on wounds and perilesional skin?”), alginate and zinc oxide deserve a post together because we combine them so much in the practice:)
Why is the combination of zinc oxide and alginate of interest?
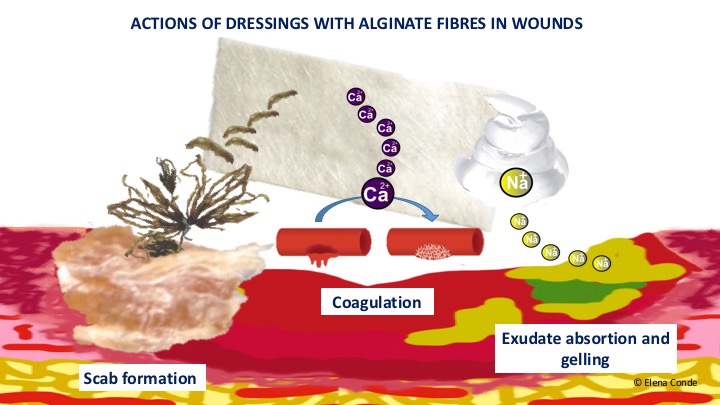
Alginate is a polysaccharide formed by mannuronic acid and guluronic acid units. It has demonstrated biocompatibility, non-toxicity, non-immunogenicity, biodegradability, hemostatic activity and can simply gel. When dried it can simulate a “scab effect” that will promote underlying epithelialization.
Although the exact mechanism of zinc in wound healing is unknown, as it is essential for the activity of many enzymes, it appears to be involved in cell replication and migration, protein synthesis, cell repair and autolytic debridement. It has also been associated with an anti-inflammatory and antimicrobial effect.
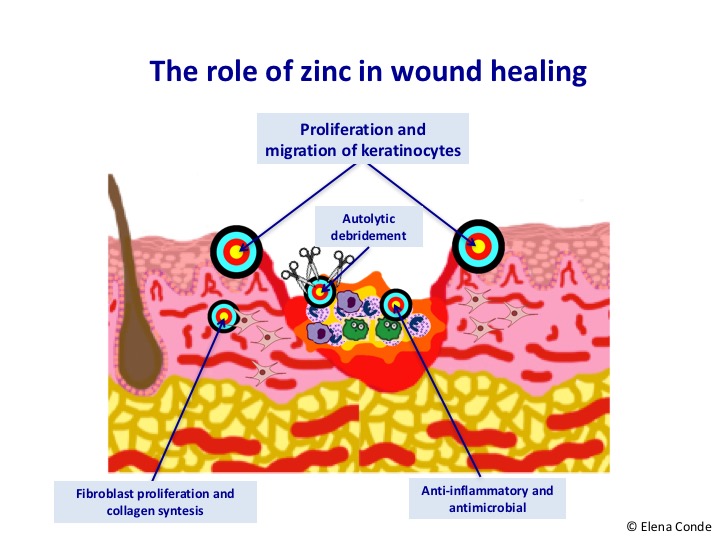
Zinc oxide allows a sustained release of zinc while avoiding cytotoxic levels. It seems to simulate the action of certain growth factors, as well as increasing their release.
Bandages combining alginate and zinc oxide have been developed, with improved healing and reduction of bacterial flora (see article).
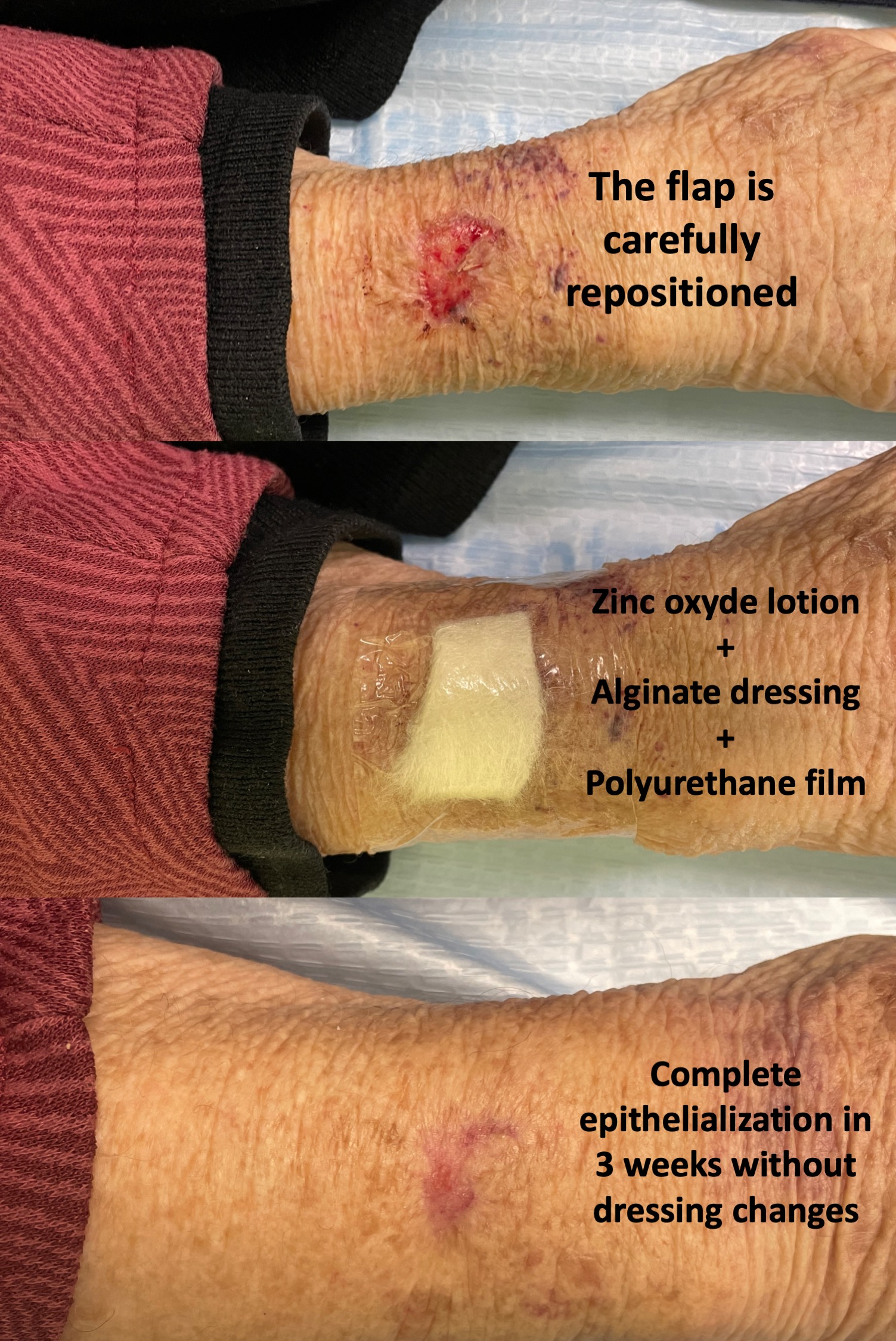
But this combination can also be done in the office, using products with zinc oxide and calcium alginate sheets. Although the best known pharmaceutical form of zinc oxide is in a paste, as a barrier product, in exudative lesions we will use an aqueous base, due to its drying action. Before applying zinc oxide lotion, it must be shaken, as it does not dissolve in water.
In what situations do we use this combination in our wound practice?
In all those cases in which we need to control inflammation, promote epithelialization, control exudate and promote a scab effect. That is to say, among its main uses are:
– Acute, superficial, uncomplicated wounds. An example is the graft donor site, a type of wound that we produce every day in the office, or traumatic wounds, such as skin tears.
–Moisture-associated lesions. These superficial erosions and ulcers can appear in folds (irritative intertrigo), areas of friction and pressure (sacral and gluteal region), or in the perilesional skin due to wound exudate. If there is a high inflammatory or eczematous component, we associate topical corticosteroid.
-Friction blisters, for example, secondary to shoe rubbing or slipping of a compressive bandage. In these cases, prior to covering with zinc oxide and alginate, we puncture the blister and empty its contents while maintaining its roof. Maintaining and repositioning the detached epidermis helps to promote epithelialization and reduce pain.
–Grafted ulcers or ulcers in the epithelialization phase. This combination promotes complete eplithelialization and prevents maceration.
–Second degree superficial burns. Taking into account that burns have an excessive inflammatory component (responsible for pain, delayed healing and pathological scarring), we add medium-high potency topical corticosteroid to the combination of zinc oxide and alginate. See post: “Does it make sense to apply topical corticosteroids to improve the healing of superficial burns?”)

How do we cover the alginate sheets?
This is a very important question, since we need a fixation that allows us to space the dressings as much as possible and that does not damage the perilesional skin.
In cases of lesions associated with moisture, the ideal is not to place any occlusive dressing over the alginate, i.e. nothing or only gauze.
In case of wounds in locations other than the leg, we will use a gauze with adhesive or a polyurethane film, which will be more atraumatic, especially in fragile skin. In the leg, the coverage will be with a bandage or compression stocking (See post “Compression is key to treating leg wounds”).
The more we space the dressings, the less we will interfere in the epithelialization process and the less risk of “tearing” of the neoformed epidermis during the removal of the dressing. This is especially important in skin tears in the elderly, where we could keep the dressing on without removing it for three weeks, until complete epithelialization.
Also available in: Español (Spanish)


